On December 3rd, Electrophysiologist from First Coast Heart and Vascular, Dr. Neil K. Sanghvi, spoke at Flagler Hospital regarding AFib and the Watchman procedure.
WATCHMAN is a one-time, minimally invasive procedure for people with atrial fibrillation not caused by a heart valve problem (also known as non-valvuar AFib) who need an alternative to blood thinners.
Non-valvular Afib can mean a lifetime of blood thinners. It can also mean a lifetime of worry about issues like bleeds and falls. More than 100,000 people have left blood thinners behind with WATCHMAN.
How WATCHMAN Works
To understand how WATCHMAN works, it helps to know more about the connection between atrial fibrillation and stroke.
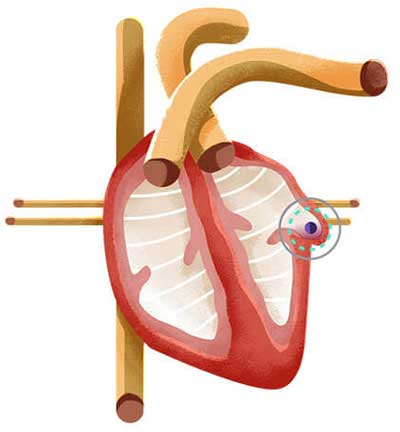
Atrial fibrillation, or AFib, affects your heart’s ability to pump blood normally. This can cause blood to pool in an area of the heart called the left atrial appendage, or LAA. There, blood cells can stick together and form a clot. When a blood clot escapes from the LAA and travels to another part of the body, it can cut off the blood supply to the brain, causing a stroke.1,2
In people with AFib not caused by a heart valve problem, more than 90% of stroke-causing clots that come from the heart are formed in the LAA.1 That’s why closing off this part of the heart is an effective way to reduce stroke risk.
The WATCHMAN Implant fits right into your LAA. It’s designed to permanently close it off and keep those blood clots from escaping. WATCHMAN is about the size of a quarter and made from very light and compact materials commonly used in many other medical implants.
Science always looks for ways to make effective treatments even better. WATCHMAN is no exception. The WATCHMAN FLX design is an advancement that enables the implant to fit a greater number of patients, giving more people than ever a safe, effective alternative to blood thinners should they need one.
In a clinical trial, 96% of people were able to stop taking blood thinners just 45 days after the WATCHMAN procedure.3
Today heart disease is America’s number one killer, but, unlike many diseases, there isn’t a specific age to start screening for heart or vascular disease. Your primary care doctor may refer you to a cardiologist if you have risk factors for cardiovascular disease or you are exhibiting symptoms that suggest that it may already be present.
Nearly half of Americans have at least one risk factor for heart disease, such as high blood pressure, obesity, physical inactivity or an unhealthy diet. Risk also increases with age.
While our First Coast Heart & Vascular physicians are your partners in heart health, you are your own best advocate. Become familiar with the risk factors and the symptoms of heart and vascular problems. Talk to your doctor if you notice changes in your health and don’t hesitate to make an appointment with one of First Coast Heart & Vascular Center’s physicians today. If you experience any of the following symptoms of heart or vascular system disease:
HEART
Angina (chest pain).
Shortness of breath.
Irregular heartbeat.
Weakness, slurred speech, dizziness, coldness, numbness or pain in the arms or legs.
Pain in the throat, jaw, neck, upper abdomen or back.
Note: Men usually have chest pain whereas women often experience extreme fatigue, shortness of breath and/or nausea.
Vascular disease deals with the circulatory system outside of your heart. Vascular disease is frequently called a silent threat since the symptoms of vascular disease may be sudden or may not present themselves at all. Talk with your physician if you have any of the risk factors shown below, to find out if you are a candidate for a vascular screening test.
Peripheral vascular disease; uncontrolled hypertension, excessive muscle cramping, limb weakness, numbness, cold feet or hands, discoloration of legs ulcers in hands or legs, claudication (pain in the legs when walking), extremity hair loss or muscle wasting, abdominal pain with eating and weight loss or swelling of the legs.
TIA (Transischemic Attack or mini-stroke)
Stroke
Pulmonary Embolism (clots in the lungs)
Clots in the legs or arms
ELECTROPHYSIOLOGY
People with heart disease may present with symptoms such as an abnormal heartbeat or arrhythmia. Some of the symptoms include:
Palpitation or “racing of the heart”
Slow heartbeat
A “fluttering” feeling in the chest
Pain or discomfort in the chest area
Lightheadedness (even fainting)
Dizziness or shortness of breath
Atrial flutter or atrial fibrillation
Extra heartbeats or PVC (premature ventricular contractions)
Graying of the skin or turning blue
SVT (Supraventricular Tachycardia)
We work in harmony with your primary care physician to deliver diagnosis and treatment of all stages of heart and vascular disease. The following are health conditions that may put you at risk for a life-changing occurrence:
Aneurysms (abdomen, arms, legs) in both arteries and veins
Atrial Fibrillation – also known as AFib or AF – is the most common arrhythmia. It affects more than 2.5 million American adults and 4.5 million people living in the European Union, and accounts for approximately one-third of hospitalizations for cardiac rhythm disturbances.
It is characterized by rapid and irregular heartbeat caused when the top chambers of the heart (the atria) quiver (fibrillate) erratically, sometimes faster than 20o times per minute.
AFib can also increase the risk of stroke fivefold. It is estimated to be responsible for 88,000 deaths and $16 Billion in additional costs to the U.S. Healthcare system. As the world population ages, the prevalence of AFib is projected to increase. In fact, in the next 30-40 years, the number of people diagnosed with AFib in the U.S. is expected to more than double.
Here’s how patients have described their experience:
“My heart flip-flops, skips beats, and feels like its banging against my chest wall, especially if I’m carrying stuff up my stairs or bending down.”
What happens during AF?
Atrial Fibrillation (AF) is the most common type of irregular heartbeat. Normally, you heart contracts and relaxes to a regular beat. In atrial fibrillation, the upper chambers of the heart (the atria) beat irregularly (quiver) instead of beating effectively to move blood into the ventricles. About 15-20 percent of people who have strokes have arrhythmia.
Additional common symptoms of atrial fibrillation
Sometimes people with AF have no symptoms and their condition is only detectable upon physical examination. Still, others may experience one or more of the following symptoms:
Rapid and irregular heartbeat
Fluttering or “thumping” in the chest
Dizziness
Shortness of breath and anxiety
Weakness
Faintness or confusion
Fatigue when exercising
Sweating
*Chest pain or pressure
*Chest pain or pressure is a medical emergency. You may be having a heart attack. Call 9-1-1 immediately.
Are there different types of AF? Do they have different symptoms?
The symptoms are generally the same; however the duration of the AF and underlying reasons for the condition help medical practitioners classify the types of AF problems.
Paroxysmal fibrillation is when the heart returns to a normal rhythm on its own. People who have this type of AF may have episodes only a few times a year or their symptoms may occur every day. These symptoms are very unpredictable and often can turn into a permanent form of atrial fibrillation
Persistent AF is defined as an irregular rhythm that lasts for longer than 7 days. This type of AF will not return to normal sinus rhythm on its own and will require some form of treatment.
Permanent AF occurs when the condition lasts indefinitely and can no longer be controlled with medication.
Over a period of time, paroxysmal fibrillation may become more frequent and longer lasting, sometimes leading to permanent or chronic AF. All types of AF can increase your risk of stroke. Even if you have no symptoms at all, you are nearly 5 times more likely to have a stroke than someone that does not have atrialfibrillation.
Know your treatment goals
The treatment goals of atrial fibrillation (AF) start with a proper diagnosis through an in-depth examination from a physician. The exam usually includes questions about your history and often an EKG or ECG. Some patients may need a thorough electrophysiology study.
Prevention and Risk Reduction
After a patient is diagnosed with atrial fibrillation, the ideal goals may include:
Restoring the heart to a normal rhythm
Reducing an overly high heart rate
Preventing blood clots
Managing risk factors for stroke
Preventing additional heart rhythm problems
Preventing heart failure
1. How will I prevent stroke?
Depending on your risk, you will likely either need aspirin or warfarin or another type of anticoagulation medication.
2.Are there additional lifestyle modifications important for stroke prevention?
3.What is my C.H.A.D.S. risk? Congestive heart failure Hypertension Age (75 or greater) Diabetes Stroke (prior episode)
4. Are there options to control my heart rate and this irregular heart rhythm?
Based on your past medical history and risk for having a future stroke, there are several options for you and your health care provider to discuss in order to manage your AF.
Medications for Atrial Fibrillation (AF)
Medications are often prescribed to prevent and treat blood clot which can lead to a stroke. The longer you have untreated AF, the less likely it is that normal rhythm can be reestablished.
Medication options may include blood thinners, rate controllers, and rhythm controllers. Lists included here are not intended to be comprehensive, and we encourage you to contact our office to keep up with the newest in AF medication options.
Preventing Clots with Medication (antiplatelets and anticoagulants)
Drugs such as blood thinners are given to patients to prevent blood clot formation or to treat an existing blood clot. Examples include Aspirin, Warfarin and other FDA Approved anticoagulants.
Important Precautions when taking anti-clotting medications
Call your healthcare provider right away if you have any unusual bleeding or bruising
If you forget to take your daily anticoagulant dose, Don’t take an extra one to catch up! Follow your healthcare provider’s directions about what to do if you miss a dose.
Always tell your doctor, dentist and pharmacist that you take one of these medicines.
Many drugs change the effects of these agents on the body. Even vitamins (and some foods) could change this effect.
Heart Rate Controlling Medication
Beta blockers, Calcium blockers and Digoxin are drugs used to slow the heart rate. Most people can function and feel better if their heart rate is controlled. Some examples may include Carvedilol, Metoprolol, Atenolol, Dilitazem, and Verapamil.
Heart Rhythm Controlling Medications
Once your heart rate is under control, the next management consideration is usually treating the abnormal heart rhythm with medications to restore the heart rhythm to normal. Your healthcare provider will most likely want to monitor progress closely. Examples include Flecainide (Tambocor), Propafenone (Rhythmol), Amiodarone, Carodarone or Pacerone, Sotalol (Betapace), or Dronedarone (Multaq).
The decision to use electrical cardio version
Your provider may recommend a trans esophageal Echocardiogram (TEE) as a first step. The TEE procedure involves swallowing a small ultrasound device that allows the healthcare team to look inside your heart atria for blood clots.
Radiofrequency Ablation or Catheter Ablation
Catheter ablationis an atrial fibrillation treatment that is done by a specialized cardiologist, called an Electro physiologist (EP) who deals with irregular heartbeats (arrhythmias).
It is a minimally-invasive procedure that is generally less invasive than surgery. It is a commonly-used treatment for atrial fibrillation as well as other cardiac arrhythmia. Like other atrial fibrillation treatments, it is most successful in treating paroxysmal atrial fibrillation, but much progress has been made in treating persistent and long standing persistent as well.
Ablation is used for cardiac arrhythmias when long-term medications or electrical cardio version are either not preferred or were not effective. Or when the patient prefers no to take any medications. Before ablation surgery, electrical mapping of the heart is performed. An electrically sensitive catheter is used to map the heart muscle and the origins of the “extra” electrical activity throughout the heart. The map tells the physician which areas of the heart are creating problematic electric signals that interfere with the proper rhythm. After a single procedure, more than 60-70% of patients with an otherwise normal heart can enjoy freedom from arrhythmias according to studies that have followed patients typically for one year. With two or more procedures, the efficacy can be as high as 80-90% in other recent case studies.
Catheter ablation is the only cardiac procedure that can be correctly called curative (No, stents are not curative)
How is an ablation performed?
A catheter (thin, flexible tube) is inserted into the patient’s blood vessels and is gently guided to the heart. The physician carefully destroys malfunctioning tissue using the catheter to deliver energy (such as radiofrequency, laser or cryotherapy) to scar the problematic areas. The scarred areas will no longer send abnormal signals. If successful, the heart will return to a normal rhythm. This minimally invasive procedure usually has a short recovery period. Patients are generally placed on a short course of anti-arrhythmic drugs while the procedure takes full effect.
Common types of Ablation include:
Pulmonary vein isolation ablation (PVI ablation or PVA) In some AF patients, fibrillation is triggered by extra electrical currents in the pulmonary veins. During this procedure, the catheter tip is used to destroy the tissue that is sending the extra currents and, in most cases, normal heart rhythm returns.
AV node ablation with pacemakers. In other AF patients, the trigger for their AF occurs in the AV node (the place where the electrical signals pass from the atria to the ventricles). The catheter is placed near the AV nod and a small area of tissue is destroyed. A pacemaker is then implanted to restore and maintain the heart’s normal rhythm.
At First Coast Heart & Vascular Center, our group treats atrial fibrillation conservatively with medical treatment, however for select cases our board certified electrophysiologist, Dr. Dinesh Pubbi can perform Atrial Fibrillation ablations at the hospitals that have state of the art EP labs.
Thank you for visiting!
Did you find what you were looking for?
Please contact us at 904-342-8300 to find out more about our practice or to schedule an appointment with any of our cardiologists.